Sesamoiditis is a painful inflammation of the sesamoid apparatus. It is characterised by pain at the first metatarsal sesamoid, commonly occurring in combination with a fixed or mobile plantarflexed 1st metatarsal.
This condition has been reported to present as often as in 4% of overuse type foot injuries1. The sesamoid complex, is reported to transmit 50% of body weight and more than 300% during push-off in the gait cycle, and is susceptible to numerous pathologies 2,3. The presence of a flexible plantarflexed 1st metatarsal can be a predisposing factor for Sesamoiditis (Potter etal1992).4
Sesamoiditis may present as often as in 4% of overuse type foot injuries1. The sesamoid complex, is reported to transmit 50% of body weight and more than 300% during push-off in the gait cycle, and is susceptible to numerous pathologies 2,3. The presence of a flexible plantarflexed 1st metatarsal can be a predisposing factor for Sesamoiditis (Potter etal 1992)4.
The sesamoids are embedded in the flexor hallucis brevis tendon and act like pulleys, exerting pressure from the big toe against the ground, aiding in the act of walking during the toe-off phase of gait. They not only have to endure the pressure of body weight and gravity, but also the constrictive pressure of the flexor hallucis brevis tendon. Sesamoids provide a smooth surface over which the tendons slide, thus increasing the ability of the tendons to transmit muscle forces, whilst in the forefoot they also assist with weight bearing and help elevate the bones of the great toe.
Repetitive chronic pressure and tension on the 1st MTPJ (particularly where a plantarflexed 1st is present) can cause the sesamoid apparatus to become irritated and inflamed. In some cases, the sesamoids may bifurcate or present as multipartite, and in severe cases, necrosis may occur due to loss of blood flow to the sesamoids.
ASSESSMENT
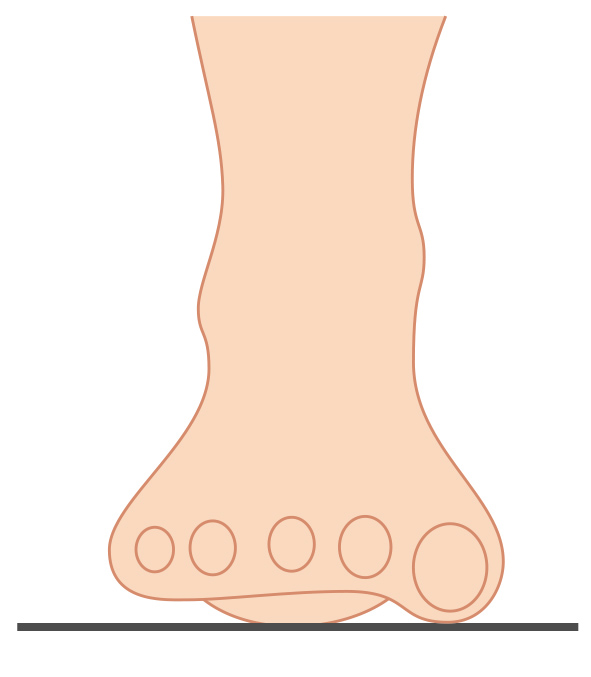
Practitioners should always check the patient for a mobile or fixed plantarflexed 1st metatarsal using the common test (Watch Video). This test will identify if there is limitation in the joint’s range of motion due to a fixed osseous condition. Palpation of the sesamoid apparatus can be undertaken to confirm if Sesamoiditis condition is present.
When a patient presents with excessive pronation or HAV (bunion), the sesamoids displace laterally, and eventually end up in the interspace between the 1st and 2nd metatarsals6, causing trauma to the sesamoid apparatus. A patient’s gait can alter as they try to compensate by weight shifting to the lateral aspect of the foot and may result in a biomechanical chain reaction causing upper body compensatory effects, such as hip pain.
Assess for Plantarflexed 1st Metatarsal
TREATMENT
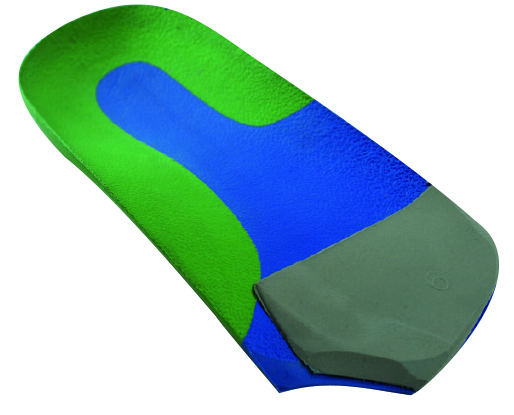
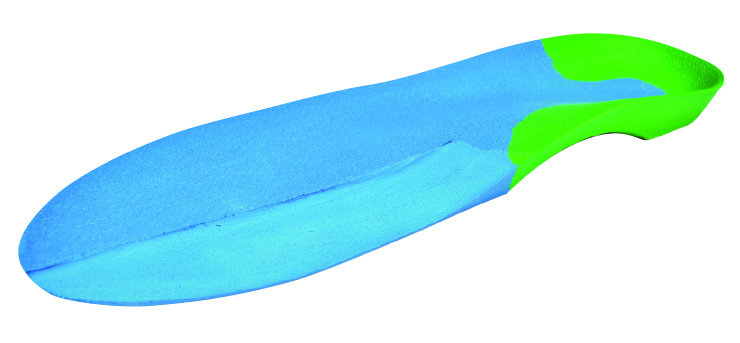
Is usually non-invasive and includes orthotic therapy to treat the pronation factor. When a fixed or mobile plantarflexed 1st metatarsal is present, modify the orthotic device with a 1st metatarsal deflection to enable off-loading of the joint. For a 2/3 length orthotic, apply a forefoot wedge to the distal edge as shown below to create a 2-5 bar, & make a crescent shape cut-out underneath the 1st Metatarsal head. For a full length device, use a hand grinder to grind a ‘trench’ relief to provide off-loading of the joint; commence grinding proximal to the 1st MTPJ and finishing at the distal edge of the full length orthotic (see below). Once the deflection is placed in the orthotic the in-built forefoot support under the 2nd to 5th metatarsals should support this area similar to a ‘2-5 bar’.
Additionally, strapping or kinesio tape can be used to immobilise the joint and allow healing to take place. Acupuncture can also be utilised to reduce inflammation.
2/3 Length Orthotic with 1st Ray Cutaway & 2-5 Bar
1. Dennis KJ, McKinney S: Sesamoids and Accessory Bones of the Foot, Clin Pocl Med Surg 7:717-723, 1990 2. Dedmond B, et al. The Hallucal Sesamoid Complex. Journal American Academy Orthopaedic Surgery 2006;14:745–53. Q15 3. Sanders T, Rathur S. Imaging of Painful Conditions of the Hallucal Sesamoid Complex and Plantar Capsular Structures of the First Metatarsophalangeal Joint. Radiology Clinic North America 2008; 46:1079–92 4. Tollarfield and Merriman. Clinical Skills in Treating the Foot, 1997 p358 5. Sharma, Punit, Singh, Harmandeep, Kumar, Rakesh. Sesamoiditis as Cause of Metatarsalgia.. Indian Journal of Nuclear Medicine. 2012 Jan-Mar; 27(1): 45–47. 6. Merriman’s Assessment of the Lower Limb 3rd Ed. Churchill Livingston; 2009, p331