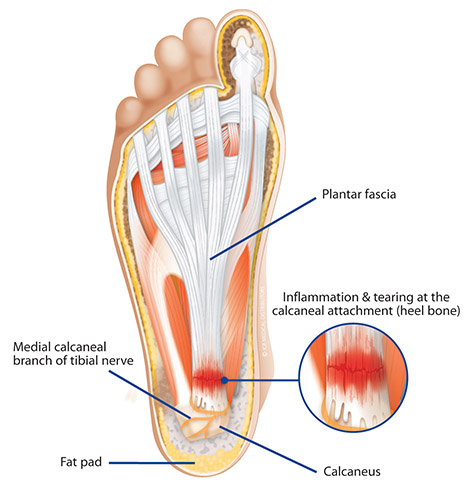
Plantar Fasciitis is inflammation caused by excessive stretching of the plantar fascia.
The plantar fascia is a broad band of fibrous tissue that runs along the the plantar (bottom) surface of the foot. The plantar fascia is attached to the calcaneus (heel) and supports the arch by acting like a bow string. When the plantar fascia is stretched excessively (often due to excessive pronation), it can cause the fascia to start to tear away from the calcaneal attachment resulting in inflammation and pain.
If left untreated, a secondary compensation of plantar fasciitis is the development of a heel spur. A heel spur develops as a bony growth on the anterior aspect of the calcaneus (front of the heel bone). It is the body’s natural response to prevent the fascia from detaching at the calcaneus. Generally a heel spur grows as a rate of approximately 1mm per year, if the stress on the plantar fascia is not relieved.
Biomechanical Aetiology
Plantar fasciitis is generally the result of faulty biomechanics. Excessive pronation, or a high strike angle supinated foot structure, can cause the plantar fascia to elongate and tear at the attachment to tuberosity of the calcaneus.
Excess subtalar joint pronation lowers the arch structure and as the foot elongates, a traction force is placed on the plantar fascia. These tractional forces can result, over time, in inflammation of the fascia and surrounding tissues, thus causing pain in the arch and heel. If chronic traction of the plantar fascia from the calcaneal tuberosity occurs, then this may lead to the development of a bony growth on the calcaneal tuberosity. The resultant projection or bone growth may be called a ‘spur’ – referred to as a ‘heel spur’ – which can be visible on X rays. Plantar fasciitis is generally a precursor to a heel spur.
Restriction of dorsiflexion of the foot through the presence of tight calf muscles can often add to plantar fascial pain due to restriction in dorsiflexion of the foot during the propulsive phase of gait. When these factors are combined with excess pronation, this results in the foot dorsiflexing at the midtarsal joint which in turn places an extra strain on the plantar fascia.
Symptoms
Sharp pain, stiffness and aching are very common with this ailment. Patients often present with a dull to sharp pain occurring about the plantar calcaneal area when getting out of bed of a morning. The plantar fascia is more inflexible at those times or when arising from a seated position and continuing during the initial periods of weight bearing. Usually the pain subsides within a few minutes, but may re-occur once this sequence is re-established. The pain is often described by patients as a ‘stone bruise’. Pain can be located at the inferior aspect of the heel either medially, laterally or centrally.
Plantar Fasciitis is more common in overweight patients, pregnant women, people who have recently increased their level of activity.
Treatment
Plantar fasciitis is most successfully treated by realigning the biomechanical structure. To do so, ICB Orthotics should be prescribed and fitted to the patient as they are designed to control excessive subtalar joint pronation which will assist in preventing over-stretching of the plantar fascia, thus relieving pain and discomfort, and preventing the condition from deteriorating and causing a heel spur to develop.
Additional Treatment
As a short term treatment, the Low Dye strapping technique can be used to relieve pain and discomfort. Low Dye strapping supports the foot and assists in correcting pronation – almost mimicking the support offered by ICB Orthotics. Usually, immediate pain relief is experienced, however a major reduction in symptoms will often be achieved within 24-72 hours.
Acupuncture and foot mobilisations may also aid in short term pain relief, as can non steroidal anti-inflammatory medications.